
Opiate withdrawal is one of the most challenging physiological and neurological processes a person can experience during recovery from opioid dependence. While it is often described in terms of physical discomfort and emotional distress, the true core of opiate withdrawal lies within the brain itself. From disrupted neurotransmitter systems to altered stress circuits and impaired reward processing, opiate withdrawal represents a profound neurological recalibration. Understanding opiate withdrawal through a neuroscience lens not only explains why symptoms can feel overwhelming, but also why medically informed, brain-based treatment is so critical for long-term recovery.
How Opiates Rewire the Brain
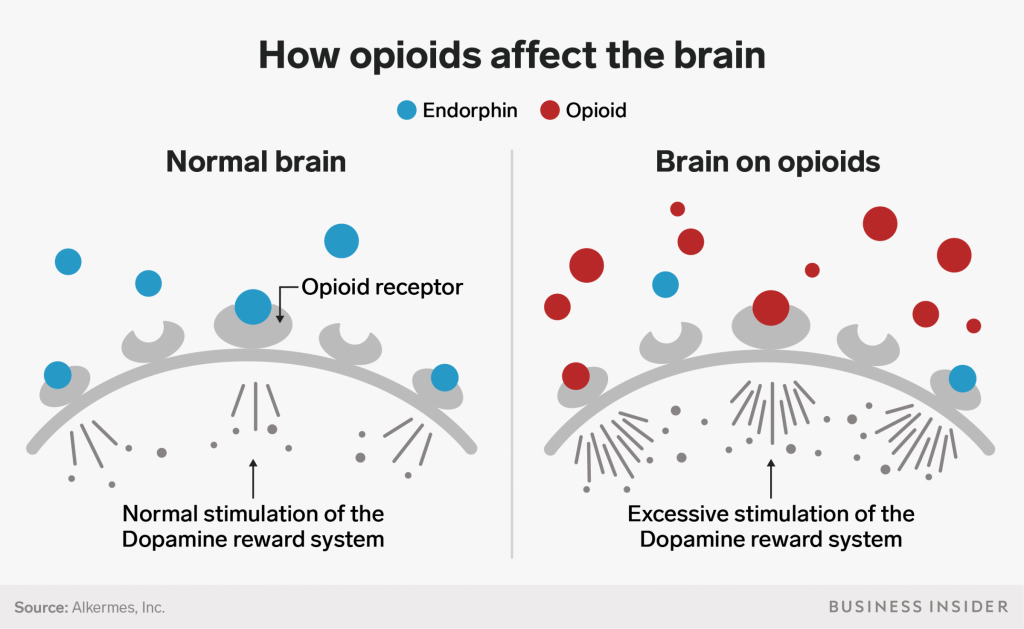
To understand opiate withdrawal, it is essential to first understand how opiates affect the brain during active use. Opiates bind primarily to mu-opioid receptors located throughout the central nervous system, particularly in areas responsible for pain modulation, reward, motivation, and emotional regulation. When these receptors are activated, they inhibit the release of neurotransmitters involved in pain signaling while simultaneously increasing dopamine activity in the brain’s reward circuitry.
Repeated exposure to opiates causes the brain to adapt. Neurons reduce their natural opioid production, opioid receptors become less responsive, and downstream signaling pathways are altered. Over time, the brain recalibrates its baseline functioning around the presence of the drug. This process, known as neuroadaptation, is the foundation of dependence and the driving force behind opiate withdrawal once drug use stops.
The Dopamine System and Opiate Withdrawal
Dopamine plays a central role in motivation, pleasure, and reinforcement learning. During opiate use, dopamine release in the mesolimbic pathway is artificially elevated, creating intense feelings of relief and reward. As dependence develops, the brain compensates by reducing dopamine receptor sensitivity and baseline dopamine production.
When opiate use suddenly stops, dopamine signaling drops far below normal levels. This dopamine deficit is a hallmark of opiate withdrawal and explains many of its psychological symptoms. Individuals often experience profound anhedonia, depression, lack of motivation, and emotional numbness. From a neuroscience perspective, the brain is not failing; it is struggling to restore balance after prolonged chemical manipulation.
The Role of the Locus Coeruleus in Withdrawal Symptoms
One of the most important brain regions involved in opiate withdrawal is the locus coeruleus. This small but powerful structure in the brainstem regulates norepinephrine, a neurotransmitter involved in arousal, alertness, and the stress response. Under normal conditions, opiates suppress activity in the locus coeruleus, producing calmness and sedation.
With chronic opiate use, the locus coeruleus adapts by increasing its baseline activity. When opiates are removed, this system rebounds aggressively, releasing excessive amounts of norepinephrine. This neurological overactivation is responsible for many classic opiate withdrawal symptoms, including anxiety, agitation, insomnia, sweating, elevated heart rate, and high blood pressure. The intense “fight or flight” sensation experienced during opiate withdrawal is rooted directly in this dysregulated stress circuitry.
Pain Processing and Hyperalgesia During Opiate Withdrawal
Opiate withdrawal is often described as intensely painful, even in individuals who did not originally use opioids for chronic pain. Neuroscience explains this through a phenomenon called opioid-induced hyperalgesia. Long-term opioid exposure sensitizes pain pathways in the spinal cord and brain, making the nervous system more reactive to pain signals.
During opiate withdrawal, the absence of opioid receptor activation unmasks this heightened sensitivity. Pain signals that were previously dampened become amplified, leading to muscle aches, joint pain, headaches, and a generalized sense of physical misery. This pain is not imagined; it reflects real neurobiological changes in pain processing circuits that take time to normalize.
The Stress Axis and Cortisol Dysregulation
Opiate withdrawal also disrupts the hypothalamic-pituitary-adrenal axis, the brain’s primary stress regulation system. Chronic opioid use suppresses cortisol release, altering the brain’s ability to respond appropriately to stress. When opioids are removed, cortisol levels often surge unpredictably.
This dysregulation contributes to irritability, mood swings, fatigue, immune suppression, and sleep disturbances during opiate withdrawal. From a neuroscience standpoint, the brain is relearning how to regulate stress without chemical assistance. This process can take weeks or months, which is why individuals may continue to feel emotionally fragile even after acute withdrawal symptoms subside.
Gastrointestinal Symptoms and the Enteric Nervous System

Opiate withdrawal is well known for causing nausea, vomiting, diarrhea, and abdominal cramping. These symptoms originate in the enteric nervous system, often referred to as the “second brain.” The gastrointestinal tract contains its own network of neurons rich in opioid receptors.
During opioid use, gut motility is suppressed. When opiates are removed, this system rebounds with excessive activity, leading to rapid intestinal contractions and digestive distress. The brain and gut communicate constantly through the vagus nerve, meaning gastrointestinal discomfort during opiate withdrawal can further intensify anxiety and emotional distress through bidirectional neural signaling.
Sleep Architecture Disruption in Opiate Withdrawal
Sleep disturbances are among the most persistent symptoms of opiate withdrawal. Neuroscience research shows that opioids significantly alter sleep architecture, particularly rapid eye movement sleep and deep slow-wave sleep. During withdrawal, the brain struggles to restore normal sleep cycles.
Insomnia, fragmented sleep, vivid dreams, and night sweats are common as neurotransmitter systems involving serotonin, norepinephrine, and gamma-aminobutyric acid remain dysregulated. Poor sleep further impairs emotional regulation, decision-making, and impulse control, increasing vulnerability to relapse during early recovery.
Neuroplasticity and Brain Recovery After Opiate Withdrawal
One of the most hopeful aspects of viewing opiate withdrawal through a neuroscience lens is understanding neuroplasticity. The brain is remarkably adaptive and capable of healing. While opiate withdrawal reflects a brain in distress, it also represents the beginning of neurological recovery.
Over time, opioid receptors regain sensitivity, dopamine signaling stabilizes, stress systems recalibrate, and pain pathways normalize. This process is gradual and influenced by genetics, duration of opioid use, overall health, and the presence of supportive treatment. Neuroscience confirms that recovery is not merely psychological; it is a measurable biological process unfolding within neural circuits.
Why Opiate Withdrawal Feels Overwhelming
From the outside, opiate withdrawal may appear to be a collection of uncomfortable symptoms. From the inside, it is a full-scale neurological reboot. Multiple brain systems responsible for reward, stress, pain, sleep, digestion, and emotion are all recalibrating simultaneously. The intensity of opiate withdrawal is a reflection of how deeply opioids integrate into core survival circuits in the brain.
This understanding helps reduce shame and stigma. Opiate withdrawal is not a failure of willpower. It is the predictable outcome of neuroadaptation and dependence, driven by well-documented changes in brain function.
The Importance of Medically Informed Withdrawal Support
Because opiate withdrawal involves complex brain systems, medically informed care can significantly reduce suffering and risk. Certain medications work by stabilizing opioid receptors, modulating norepinephrine release, or supporting sleep and stress regulation. From a neuroscience perspective, these interventions help the brain transition more safely back toward equilibrium rather than forcing an abrupt and overwhelming recalibration.
Supportive environments also play a critical role. Reduced sensory stress, proper nutrition, hydration, and emotional safety all influence neural recovery. The brain heals best when it is not simultaneously battling chaos, fear, or exhaustion.
Long-Term Brain Changes Beyond Acute Opiate Withdrawal

Even after acute opiate withdrawal resolves, lingering neurobiological effects may persist. Post-acute withdrawal involves ongoing dopamine dysregulation, heightened stress sensitivity, and impaired executive function in the prefrontal cortex. These changes can affect decision-making, emotional control, and craving regulation.
Neuroscience emphasizes that continued treatment, therapy, and brain-supportive interventions are not signs of weakness but necessary steps in restoring full neural health. Recovery is not simply the absence of opiate withdrawal symptoms; it is the gradual rebuilding of resilient brain networks.
A Neuroscience-Based View of Hope
Viewing opiate withdrawal through a neuroscience lens transforms the recovery narrative. The symptoms are not random, punitive, or endless. They are signs of a brain working tirelessly to regain balance after prolonged disruption. With appropriate care, time, and support, the same neuroplastic mechanisms that once reinforced dependence can be harnessed to support healing and long-term recovery.
At Neuroscience Research Institute, understanding the brain is central to understanding recovery. Opiate withdrawal is not the end of the story; it is the brain’s first step toward restoring health, resilience, and self-regulation.
